
Modernizing a legacy LIMS (Laboratory Information Management System) is no longer optional for genomics and diagnostics organizations; it's a matter of operational survival.
A 2024 Deloitte survey found that 92% of genomics labs cite LIMS modernization as their top digital transformation priority, yet 63% report failed attempts or major disruptions during migration, primarily due to poor planning, compliance gaps, and lack of architectural foresight.
The reality is simple:
- Legacy LIMS systems were not designed for today’s volume of sequencing data, integration requirements, or compliance expectations.
- Modern genomics workflows require cloud-native infrastructure, robust auditability, and streamlined interoperability across lab, compute, and clinical systems.
Yet many labs approach modernization like a simple IT upgrade. They treat it as “moving data to a new platform,” rather than rebuilding the foundation for an evolving genomic enterprise.
This is where projects fail and costs explode.
In this guide, we’ll walk through:
- Why LIMS modernization is uniquely difficult in genomics
- The core architectural and compliance principles you must get right
- A step-by-step modernization roadmap used by high-performing labs
- Common pitfalls and how to avoid them
- How to decide whether to build, buy, or adopt a hybrid model
Why Legacy LIMS Systems Break in Genomics
LIMS platforms originally emerged to manage sample tracking, lab inventory, and operational workflows. In traditional clinical labs, they handled predictable data types and linear processes. Genomics changes everything:
Massive file sizes
FASTQ, BAM/CRAM, VCF, QC reports
Complex pipelines
multi-stage computational workflows, reproducibility requirements
Interoperability demands
sequencers, bioinformatics tools, EHR systems, payer systems, reporting tool
Compliance scope
HIPAA, CLIA, CAP, SOC 2, GDPR and genetic privacy regulations
Scientific evolution
assays, pipelines, and interpretation logic change continuously
Most legacy LIMS systems cannot adapt to these dynamics. Their data models are rigid, integration layers are brittle, and auditability is often weak.
The Three Hidden Risks of LIMS Modernization
A lab cannot “pause” operations. If your modernization effort disrupts sample tracking, instrument connectivity, or reporting, it impacts turnaround time, revenue, and patient outcomes.
If your new architecture fails a HIPAA risk assessment, SOC 2 audit, or CLIA/CAP validation, the project is not just delayed, it may become unusable in clinical environments.
Many labs modernize by purchasing a COTS LIMS and customizing it. They later discover that:
- Customization costs balloon,
- Integration timelines stretch,
- And switching platforms becomes nearly impossible.
Alternatively, labs build custom systems and become dependent on a small internal engineering team. When key developers leave, the platform becomes unmaintainable.
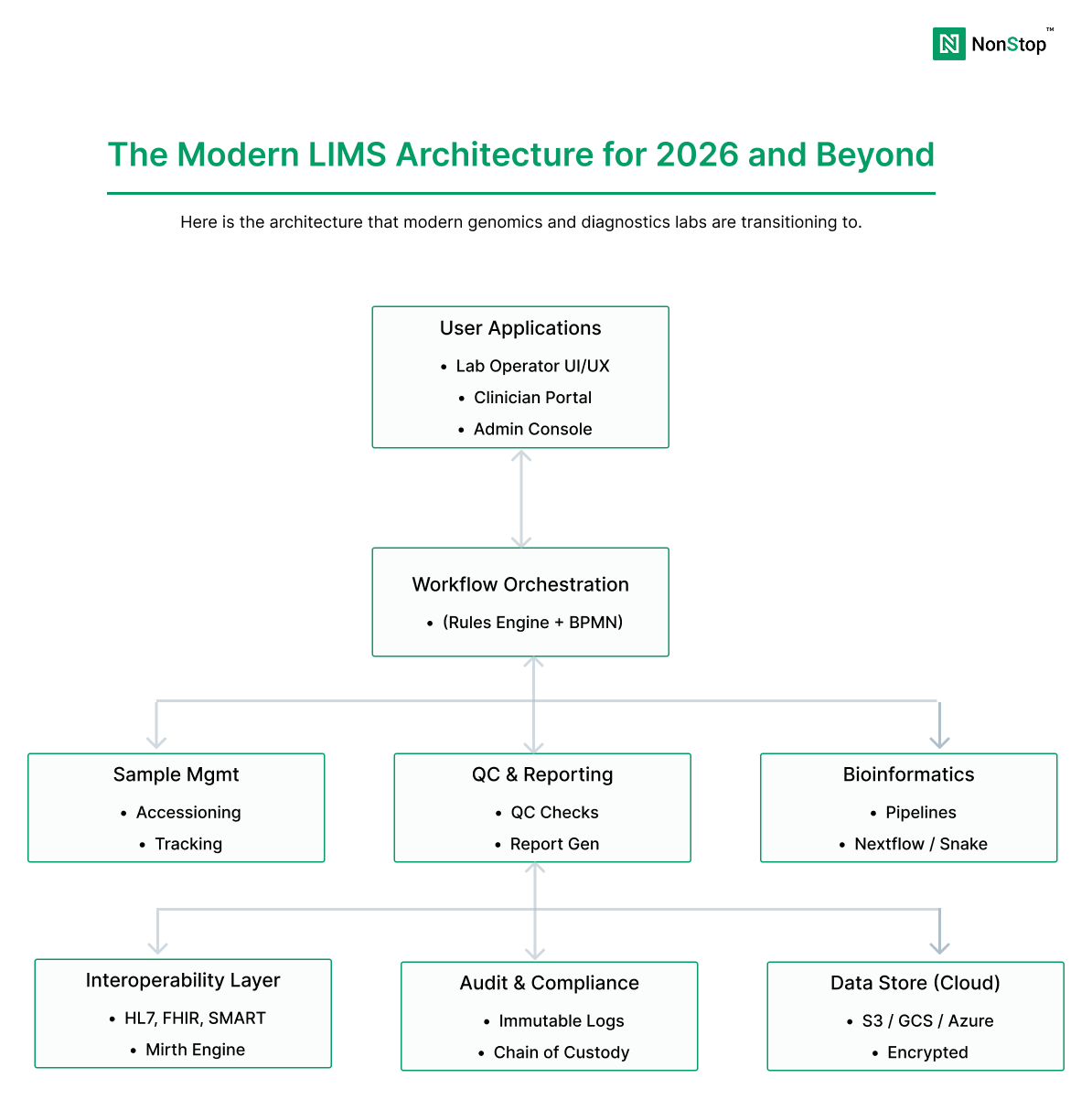
The Modern Genomics LIMS Architecture: What “Good” Looks Like
A modern LIMS platform for genomics typically separates concerns into distinct layers:
sample accessioning, QC, chain of custody, batching, instrument integration
pipeline orchestration, compute, reproducibility, outputs
annotation, scoring, clinical interpretation, report generation
EHR, billing, partner portals, CROs, data exchange standards (HL7/FHIR)
audit logs, access controls, monitoring, incident response readiness
This modular architecture allows labs to modernize incrementally, replace components without re-validating the entire system, and scale compute and storage independently.
A Practical LIMS Modernization Roadmap (Step-by-Step)
Define your scope and modernization goals
Start by clarifying what you are modernizing and why.
Key scope questions
- Are you replacing the entire LIMS or only modernizing key modules?
- Is the goal operational efficiency, scalability, compliance, or interoperability?
- Are you building a clinical genomics platform or a research-focused system?
- What is your target turnaround time, throughput, and assay pipeline roadmap?
Inventory workflows and data flows (before you touch code)
Most modernization failures occur because teams underestimate workflow complexity.
Document:
- Sample lifecycle workflows (accessioning → QC → batching → sequencing → analysis → reporting)
- Instrument and sequencer integrations
- Pipeline orchestration and compute dependencies
- EHR and partner integrations
- Manual workflows that exist today
Classify data and establish PHI boundaries
A genomics LIMS almost always contains PHI because sample identifiers, patient metadata, and genomic files can be re-identifiable.
Data Type
Classi
fication
Moderniz
ation Implication
Patient demog
raphics
PHI
Requires strict access control and audit logs
FASTQ/
BAM/
CRAM
PHI / Identifiable
Must be isolated in secure processing zones
VCF + clinical metadata
PHI
Requires encryption at rest/in transit; PHI-safe logs
Aggregated statistics
Non-PHI (if de-identified)
Can support analytics without PHI exposure
Choose your modernization strategy (build, buy, or hybrid)
Most genomics organizations end up in a hybrid model: buy core utility functions, build differentiated workflows and integrations.
Design for interoperability (EHR + instruments + partners)
Modern LIMS platforms must integrate seamlessly with:
- Sequencers and instruments (Illumina, Thermo, etc.)
- Pipeline orchestration systems (Nextflow, Cromwell, Airflow)
- Clinical EHR systems (Epic, Cerner) via HL7/FHIR
- Billing and payer systems
- Partner portals and CRO data exchange
The integration layer is often where modernization either succeeds or fails.
Implement compliance-by-design (not compliance-after)
Compliance is not a checklist you add at the end. You must architect for:
- Role-based access control (RBAC) and least-privilege IAM
- Centralized, immutable audit logs
- Encryption at rest and in transit
- Secure pipeline execution zones
- PHI-safe observability (no PHI in logs)
- Validation protocols (CLIA/CAP where applicable)
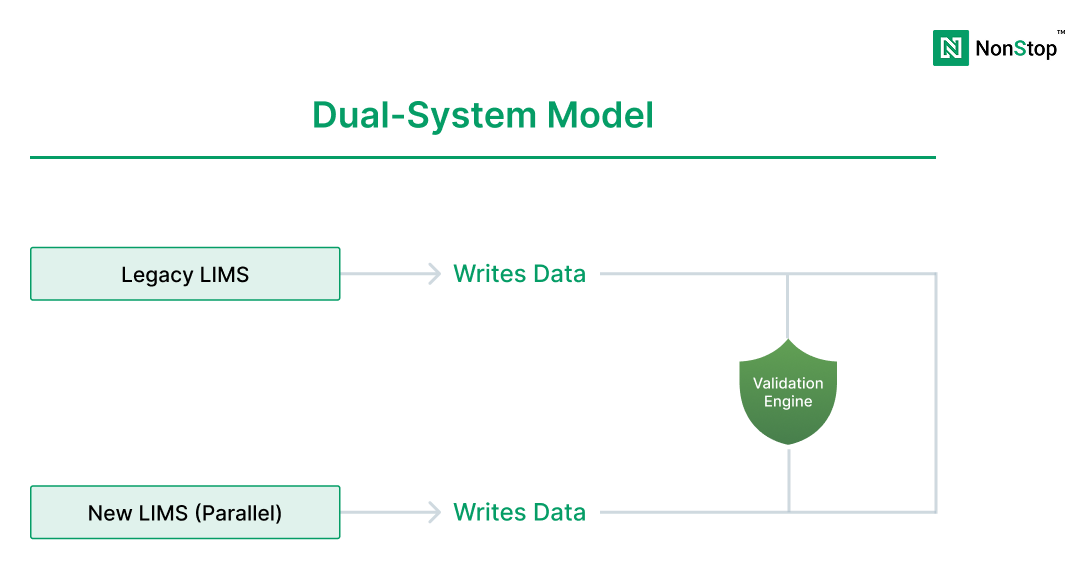
Execute migration in phases (avoid big-bang cutovers)
Big-bang cutovers are one of the biggest causes of lab disruption.
Preferred phased approach:
- Phase 1: Parallel run for sample tracking + basic workflow
- Phase 2: Add pipeline orchestration + compute integration
- Phase 3: Add reporting + EHR integration + advanced automation
- Phase 4: Decommission legacy systems only after validated stability
Common Mistakes That Derail LIMS Modernization
teams underestimate real lab behavior
leads to failed risk assessments and re-architecture
data quality issues surface late
locks teams into inflexible systems
integration delays dominate project timelines
causes compliance failures and deployment delays
This modular architecture allows labs to modernize incrementally, replace components without re-validating the entire system, and scale compute and storage independently.
Conclusion
A successful genomics LIMS modernization initiative requires more than a new UI or a database migration. It demands a full rethinking of architecture, compliance, interoperability, and operational workflows.
The labs that modernize successfully do so by:
- treating modernization as a product transformation, not an IT upgrade,
- architecting compliance and auditability from the start,
- planning phased migration to avoid lab disruption,
- and building modular systems that can evolve as science advances.